


It appears that little consistent information is available on medical interventions and the use of appropriate intensity and exercise mode to improve physiological and psychological menopause complications. The aim of this study was to compare the effect of eight weeks of low, moderate and high intensity TRX training on hot flashes, mood, fat percentage and muscular endurance of postmenopausal women. Forty non-athletic postmenopausal healthy women participated in the study and were randomly and equally divided into four groups: (1) control, (2) low-intensity TRX training (LI TRX) (40–55% HHR), (3) moderate-intensity TRX training (MI TRX) (55–70 HHR), and (4) high-intensity TRX training (HI TRX) (70–85 HHR). The research variables were measured 48h before and after the intervention. The experimental groups performed their own training program for 8 weeks, 3 sessions per week, and 60min each session. Symptoms of hot flashes, mood, fat percentage, and muscular endurance in the experimental groups significantly improved compared to the control group (P≤0.05). A decrease in fat percentage was observed in the MI TRX group compared to other training groups (P=0.045). Adaptation to regular exercise training reduced menopausal symptoms. There was no significant difference between using different intensity of exercise. Probably due to the physiological and psychological aspects of menopause, the most important factor in improving menopausal symptoms is participating in exercise and the frequency of exercise training. Also, TRX can be used as a safe method in different intensities in this group of women.
Menopause is part of the normal aging process for women, and between 74 and 80% of women are affected by menopausal symptoms. This period begins with the onset of the first signs of menopause and lasts for 5–10 years after menopause.1 As a result of menopause, ovarian estrogen decreases significantly, and the signs and symptoms of estrogen deficiency including mood swings, overweight, increased fat percentage, osteoporosis, and especially the symptoms of vasomotor (the main cause of hot flashes), nutritional disorders, etc. appear.2–7 Note that steroid hormones have a wide range of effects due to the passage of membranes in all cells of the body, and a decrease in these hormones will lead to many complications.3
Hot flashes are the most common of these symptoms, causing frequent awakenings, sleep deprivation, and physical and mental fatigue. In 10–20%, it is unbearable and in 20% it may continue for up to 15 years after menopause.5,8 The most common symptoms of hot flashes are: sudden and severe heat in the face and neck, arms and lower torso, rapid heartbeat, sweating, night sleep disturbances, headaches, anxiety, dizziness, weakness and fainting that can be seen in women.5,9 Based on the above points and regarding many changes that occur in postmenopausal women, research has been conducted on postmenopausal women, including the impact of exercise programs and physical activity. Muscle weakness in daily activities has also been reported in postmenopausal women, possibly due to decreased muscular endurance, and exercise training can reduce the symptoms of fatigue in this group of women by affecting muscular endurance.10
The physiological effects of exercise training on weight loss, decreased insulin resistance, decreased leptin, improved lipid profile, and subsequently increased cardiovascular function have been well studied in women's health and cardiovascular disease.11–13 However, little information is available on the application of different exercise patterns and intensities in menopausal conditions.
Research into the effects of physical activity on menopausal symptoms, such as hot flashes in postmenopausal women, is contradictory, with some reporting a decrease, no change or an increase in menopausal symptoms.14–16 In a study to investigate the effect of aerobic exercise on menopausal symptoms in 154 women aged 45–63, Moilanen et al. (2012) concluded that 50-min sessions of regular aerobic exercise resulted in a significant reduction in night sweats, depression, mood disorders, irritability, headache and urinary problems compared to the control group.17 Also, Luoto et al. (2012) showed that 6 months of aerobic exercise reduced nocturnal hot flashes in postmenopausal women but did not change the women's health scale; on the other hand, depressive levels decreased and participants’ respiratory heart rate and muscle mass increased significantly.18 In addition, no specific studies have been performed on modern exercise patterns that are often considered by women. One of these methods is Total body resistance exercise (TRX), which has recently been added to the body's total resistance exercise in the form of instability exercises, and the interest in using this system to improve health and improve athletic performance is increasing, especially in women in urban communities.19–23
TRX is a form of suspension training that uses body weight exercises to develop strength, balance, flexibility and core stability simultaneously. In general, TRX exercises are performed with rope or cord, in which muscle contraction occurs through the distance between the central axis of the rope and consists of two handles and a body. In addition, compared to traditional dumbbell or barbell exercises, TRX makes it more challenging to perform movements through wider angles and movements. Also, these training tools and methods are used for various purposes of general athletes’ fitness and rehabilitation. In general, suspension exercise seems to enhance the function of deep sensory receptors such as muscle spindles and the Golgi tendon organs and increase balance and stability through pressure on the abdominal muscles and pelvic floor muscles.19–23
Given the effects of menopause and the importance of reducing these symptoms through medical-sports interventions, as well as the existence of some contradictions in studies, it is important to investigate this issue. Due to the widespread effects of reduced steroid hormones, many aspects of this phenomenon remain unknown, especially in the field of sports physiology, and studies in the field of application of appropriate intensity and pattern are very scattered and decentralized. Also, most studies have focused only on reducing menopausal symptoms and paid less attention to improving physical fitness functions along with psychological factors. Besides, the novelty of TRX exercises has also made it impossible to have complete information about the advantages and disadvantages of these exercises. In addition, in the present study, an attempt has been made to collect maximum information through field methods and questionnaire so that it can be readily and easily implemented for the general public if the desired results are observed. Therefore, the aim of this study was to compare the effect of eight weeks of low, moderate and high-intensity TRX training on hot flashes, mood, fat percentage and muscular endurance of postmenopausal women.
Material and methodsThe experimental protocol in this study was approved by the ethics committee of Islamic Azad University, Central Tehran Branch (No. 10121423972026). The researchers’ Ethics Committee initially approved the experimental procedures and study protocols, which were fully explained to all participants, and a written consent form was signed after having read and understood the details of the experiments. The research was also conducted in accordance with the principles stated in the Declaration of Helsinki.
The present semi-experimental research was conducted as a field study based on pre-test and post-research research design. Regarding the research procedures, the purpose of the study first explained to the participants and after obtaining the consent of the participants, the healthy obese postmenopausal women were identified, provided that they had the inclusion criteria (i.e., not taking any hormonal drugs and underlying disease over the past six months, negative result for their Pap smear test over the past year, complaining of menopausal symptoms). Then, forty participants were equally divided into four groups of 10 subjects randomly: (1) control, (2) low-intensity TRX training (LI TRX) (40–55% HHR), (3) moderate-intensity TRX training (MI TRX) (55–70 HHR), and (4) high-intensity TRX training (HI TRX) (70–85 HHR) (Table 1). Interventions included 8 weeks of TRX training with a frequency of 3 sessions per week and a duration of 60min per session. The research variables were measured 48h before and after the interventions (Table 2).
Characteristics of the participants in the study groups.
| Groups | Control | LI TRX | MI TRX | HI TRX | ||||
|---|---|---|---|---|---|---|---|---|
| Time | Pre | Post | Pre | Post | Pre | Post | Pre | Post |
| Age | 50.4±2.35 | – | 50.30±2.75 | – | 51±2.39 | – | 50.30±2.52 | – |
| Height | 157.1±4.8 | – | 155.4±4.08 | – | 156.7±3.4 | – | 155.2±6.1 | – |
| Weight (kg) | 75.89±3.7 | 76.5±4.05 | 76.2±4.2 | 74.46±5.3 | 76.3±4.8 | 74.88±3.1 | 76.48±6.1 | 74.7±6.2 |
| BMI (kg/m2) | 30.75±1.3 | 30.79±1.4 | 31.56±1.8 | 30.84±1.4 | 31.08±0.7 | 30.49±0.7 | 31.76±1.5 | 31.02±1.5 |
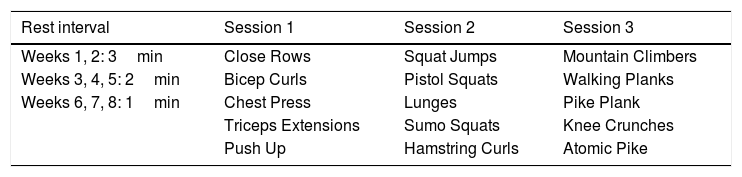
Movement patterns and rest intervals used in the training groups for each week of total body TRX training.
| Rest interval | Session 1 | Session 2 | Session 3 |
|---|---|---|---|
| Weeks 1, 2: 3min | Close Rows | Squat Jumps | Mountain Climbers |
| Weeks 3, 4, 5: 2min | Bicep Curls | Pistol Squats | Walking Planks |
| Weeks 6, 7, 8: 1min | Chest Press | Lunges | Pike Plank |
| Triceps Extensions | Sumo Squats | Knee Crunches | |
| Push Up | Hamstring Curls | Atomic Pike |
Body mass index was calculated in kg/m2 using BMI equation through measuring height (Seca 213, Germany recorded to the nearest 0.1cm) and weight (SECA Digital Scale Model 727: with precision of 2g). All subjects took the modified pull-up test to determine muscular endurance. They also completed the Kupperman Index Questionnaire24 and BRUMS,25 respectively, to determine hot flashes and mood scale. The fat percentage was calculated using the caliper (RMC, Amparo, SP, Brazil) and 3-point equation (triceps, suprailiac, thigh) of Jackson-Pollock for women. Based on the obtained measurements, the body density was calculated using the following formula.26,27
Brunel questionnaire

The Brunel questionnaire measures the six mental states mentioned in POMS and BRUNEL with 24 questions together with two other states, cheerfulness and relaxation. As a result, it consists of 8 subscales, including 32 questions and 8 sub-scales and each sub-scale has 4 questions. Also, vigor, relaxation and cheerfulness (a total of 12 questions) are the positive dimensions of mood and in contrast tension, depression, anger, fatigue and confusion (a total of 20 questions) are the negative dimensions of mood in the Brunel Mood Scale (BRUMS) questionnaire.25
Kupperman index questionnaireIn this study, the Kupperman index questionnaire was used to determine the extent of hot flashes. This indicator has been used in various studies on menopausal symptoms. The questionnaire includes eleven menopausal symptoms (hot flashes, insomnia, fatigue, depression, palpitations, headaches, joint and muscle pains, nervousness, dizziness, pricking and numbness, and a tingling sensation) each of which is given a score of zero (no symptom), one (mild symptom), two (moderate symptom), and three (severe symptom).24
Implementation of TRX trainingOne week before the start of the training protocol, the subjects were introduced to the correct way to perform techniques and movements. The training protocol included warm-up, core training, and cooling down. The movements of each session were performed in 3 sets, each set with an average of 8 repetitions at an intensity of 40–55% HRR by low intensity group (RPE 9–11), 55–70% HRR by moderate intensity group (RPE 12–13) and 70–85% HRR by high intensity group (RPE 14–17).
In order to create an overload, the rest intervals in the first and second weeks were considered 2–3min; in the third, fourth and fifth weeks were considered 2min; and in the seventh and eighth weeks were considered equal to one minute (Table 2). Among the various types of TRX exercises, those were chosen to engage most muscle groups, making them easier and more appealing for participants to perform.
All exercises were performed under the supervision of a trainer. To determine the pressure of the exercises and before the start of the protocol, the subjects were introduced to the Burg scale (6–19 standards) and its range. For example, the range of pressure perception from 14–17 on this scale was considered equal to the training pressure of 70–85%. Also, the intensity of the exercise training was controlled by different rhythms using the participants’ heart rate (Polar T31; Polar Electro, Kempele, Finland)).
The maximum heart rate was calculated using the Tanaka et al. equation (HRmax=208−(0.7×age)). The percentage of heart rate was calculated using the reserve heart rate (HRR method: Target HR (THR)=[(HRmax−HRrest)×% Intensity]−HRrest). The participants were asked to record and report their HRrest every morning. The equations and guidelines implemented were controlled according to different criteria using the ACSM guideline.26
Statistical analysisIn order to describe the data, measures of central tendency (mean), and dispersion tendency (standard deviation) and statistical diagrams were used. To test the normality of data distribution, the Spiro–Wilk test was used, also for inferential analysis of data and to eliminate the effect of pre-test, analysis of covariance (ANCOVA) and Tukey's post hoc tests at significance level P≤0.05 were used applying SPSS 21 software. Finally, Excel software was used to draw the graphs.
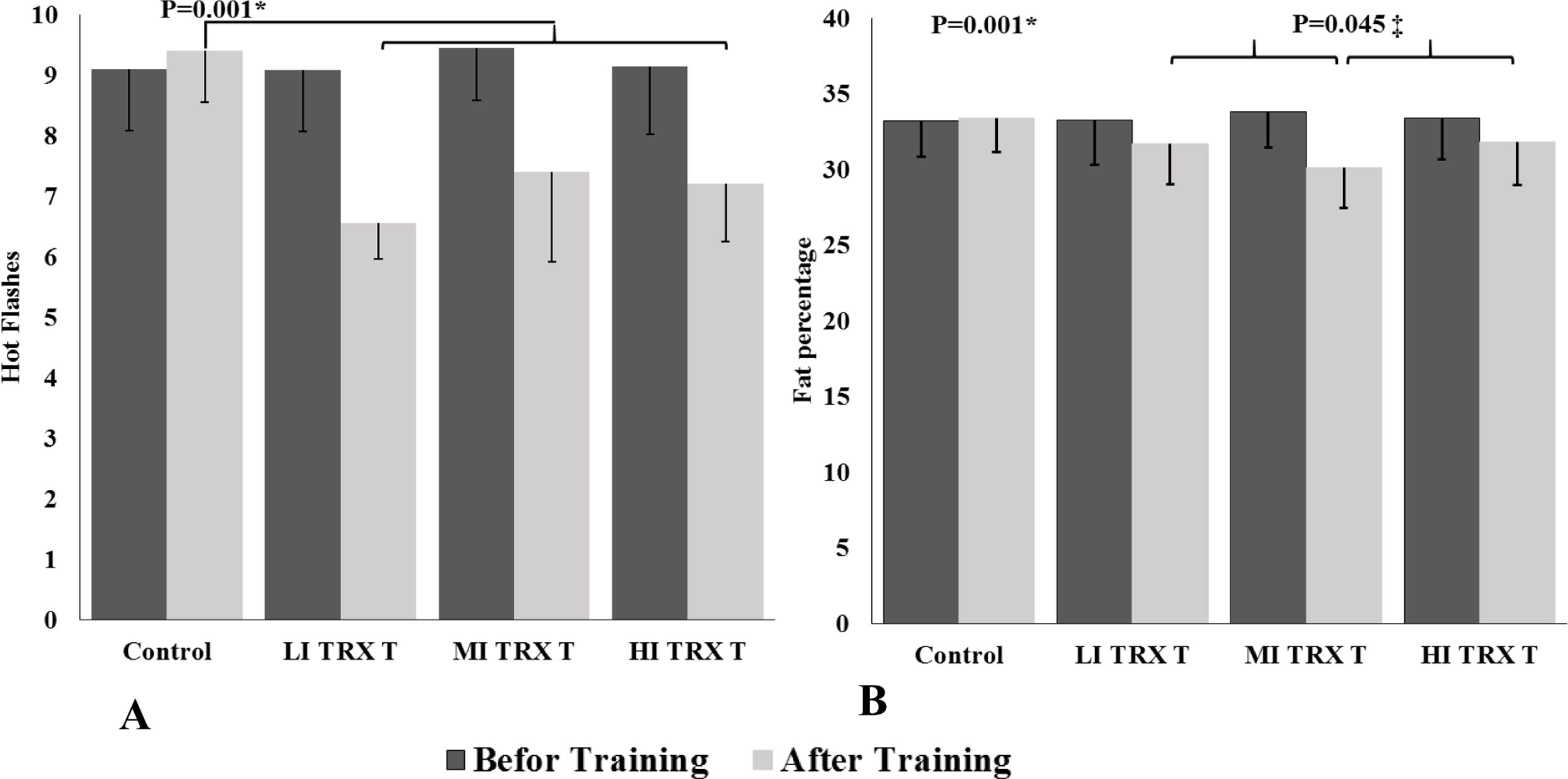
ResultsStatistical analysis of data showed that the rate of hot flashes (P=0.001, F=24.387), fat percentage (P=0.001, F=102.775) and negative mood (P=0.001, F=117.534) decreased significantly in the training groups compared to the control group. Also, positive mood (P=0.001, F=52.839) and muscular endurance (P=0.001, F=24.714) showed a significant increase in the training groups compared to the control group. Only fat percentage in the moderate-intensity training group showed a greater decrease than other training groups (P=0.045) (Table 3) (Fig. 1A and B). There was no significant difference between the training groups and the different intensities of training in other indicators. Also, despite some weight loss and body mass index, there was no significant difference between the study groups as well as compared to the pre-training period (Table 3).
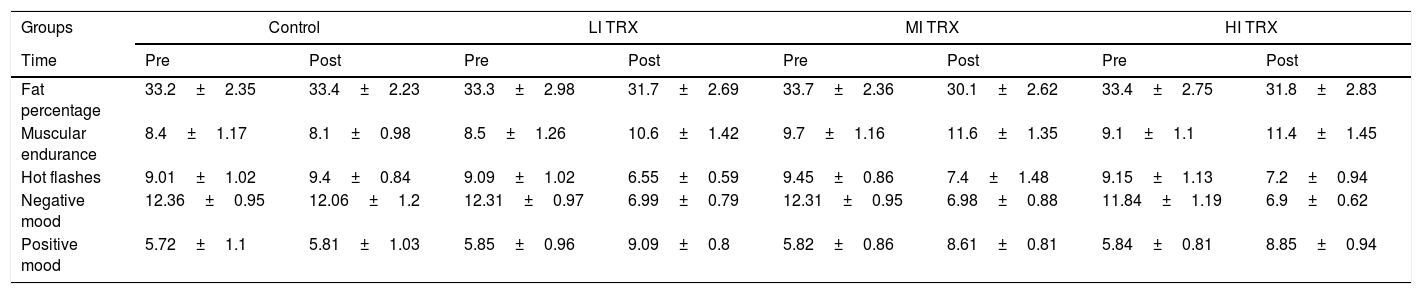
Changes in the indicators measured based on the mean and standard deviation in the study groups.
| Groups | Control | LI TRX | MI TRX | HI TRX | ||||
|---|---|---|---|---|---|---|---|---|
| Time | Pre | Post | Pre | Post | Pre | Post | Pre | Post |
| Fat percentage | 33.2±2.35 | 33.4±2.23 | 33.3±2.98 | 31.7±2.69 | 33.7±2.36 | 30.1±2.62 | 33.4±2.75 | 31.8±2.83 |
| Muscular endurance | 8.4±1.17 | 8.1±0.98 | 8.5±1.26 | 10.6±1.42 | 9.7±1.16 | 11.6±1.35 | 9.1±1.1 | 11.4±1.45 |
| Hot flashes | 9.01±1.02 | 9.4±0.84 | 9.09±1.02 | 6.55±0.59 | 9.45±0.86 | 7.4±1.48 | 9.15±1.13 | 7.2±0.94 |
| Negative mood | 12.36±0.95 | 12.06±1.2 | 12.31±0.97 | 6.99±0.79 | 12.31±0.95 | 6.98±0.88 | 11.84±1.19 | 6.9±0.62 |
| Positive mood | 5.72±1.1 | 5.81±1.03 | 5.85±0.96 | 9.09±0.8 | 5.82±0.86 | 8.61±0.81 | 5.84±0.81 | 8.85±0.94 |
 Changes in the hot flash points between the study groups. * The symptoms of hot flashes in the control group were more than the training groups after treatments (P≤0.05). (B) Changes in the body fat percentage between the study groups. * Indicates a significant reduction in fat percentage in the TRX training groups compared to the control group (P≤0.05). ‡ Indicates a significant reduction in fat percentage in the MI TRX group compared to other TRX training groups (P=0.045). The study groups include: control, low intensity TRX training (LI TRX), moderate intensity TRX training (MI TRX), high intensity TRX training (HI TRX).")
(A) Changes in the hot flash points between the study groups. * The symptoms of hot flashes in the control group were more than the training groups after treatments (P≤0.05). (B) Changes in the body fat percentage between the study groups. * Indicates a significant reduction in fat percentage in the TRX training groups compared to the control group (P≤0.05). ‡ Indicates a significant reduction in fat percentage in the MI TRX group compared to other TRX training groups (P=0.045). The study groups include: control, low intensity TRX training (LI TRX), moderate intensity TRX training (MI TRX), high intensity TRX training (HI TRX).
The results of the present study showed that there is a difference between the effect of 8 weeks of low, moderate and high-intensity TRX training on the rate of hot flashes in postmenopausal women (Table 3) (Fig. 1A). Also, the results of the post hoc test showed that there is a difference between the experimental groups and the control group, which shows the effect of all three intensities of TRX training on the amount of hot flashes, but there was no difference between the experimental groups (Table 3). Also, the highest decrease in fat percentage was observed in the TRX training group with moderate intensity (Fig. 1B).
Participation in regular exercise, frequency of exercise training, reduction of negative mood, adaptation to intensity of exercise and adrenergic system, and increased activity of endogenous opioids are probably the most important factors in the results of the present study. Because the adrenergic system has been reported to be one of the most important factors in increasing vasomotor activity. In this regard, Luoto et al. (2012) showed that nocturnal hot flashes in postmenopausal women decreased significantly after 6 months of aerobic activity, which is consistent with the results of the present study.18
The mechanisms of effect of exercise training on physiological variables such as fat percentage and muscular endurance have been well discussed and the results of the present study have confirmed this improvement in physiological performance in the training groups.11–13 Regarding muscular endurance, it should be noted that the nature of this variable is such that it is more affected by the number of repetitions, training volume and frequency of training, so it makes sense that there is no significant difference between study groups that performed TRX training with different intensities. However, no study was found in the review of literature to have examined the effect of TRX or other training programs on muscular endurance in postmenopausal women.
Since in present study the intensity control factor was the indicator of pressure perception and heart rate range was the target, in some cases the high intensity training group had a higher number of repetitions. Also, if the heart rate of each participant reached the target range even before reaching full repetitions, the set would be stopped so that everyone could perform the activities with a definite heart rate; however, on average, all participants performed 8 repetitions. In addition, the pressure perception indicator was used from time to time to ensure that the only difference was the intensity of the exercise.
Regarding the findings of the present study, we can point to the basic principles and purpose of TRX exercises. The TRX exercises are designed to strengthen endurance, physical strength, balance, flexibility, speed and agility in physical fitness. On the other hand, in connection with this finding of the present study, we can point to the relationship between strength and endurance. Muscular strength has been shown to be closely linked to muscular endurance. Muscular endurance is the ability of a muscle or group to perform a series of repetitive contractions or to produce a constant force over a period of time. As muscular strength increases, so does muscular endurance.
Decreased fat percentage in the TRX training group also indicates the effectiveness of optimal training intensity to influence physiological indicators. If the exercises are considered more or less than the intended intensity to affect each physiological indicator, their effect will be reduced.11–13 Based on the results of the present study, as well as other studies, the use of moderate-intensity training is essential to increase fat oxidation.11–13
Exercise training may also play an important role in improving psychological symptoms, especially mood, by influencing stress response mechanisms.28–30 Because menopausal symptoms are a complex combination of physiological and psychological changes, the frequency of training is likely to be the most effective factor to change other variables. The frequency of at least 3 sessions per week has been confirmed to affect mood changes and psychological disorders.15,31,32 Reduction of vasomotor activity is also one of the most important factors affecting regular exercise training to improve hot flashes symptoms by modulating the function of sympathetic nerves and the performance of beta-adrenergic receptors.28,33,34 Meanwhile, the increase in endogenous opioids caused by physical activity has a significant role in relaxing as well as moderating the activity of HPG axis. Research has shown that exercising for a long time is associated with increased levels of plasma endorphins. Increased plasma endorphin levels, in turn, reduce FSH and LH levels.35
Because high levels of FSH are the strongest and most reliable hormonal estimators for the occurrence and severity of hot flashes in women, decreased FSH levels also appear to indicate a decrease in severity and recurrence of hot flashes and vasomotor symptoms.5 However, the present study did not measure FSH levels, which is one of the limitations of the present study. But research has shown that physical activity by directly regulating FG and LH levels diminishes hot flashes by eliminating excess body heat. One of the most important factors in not distinguishing experimental groups with each other in the present study is probably the compatibility with the intensity and patterns performed.
Although the target of this effect was controlled by using the fatigue perception indicator as well as the resting heart rate and its use in calculating the heart rate, it is important to pay attention to adaptation as well as individual differences in response to exercise. Future studies can consider exercise volume as an overload by diversifying and increasing movement patterns. In this way, significant improvements and endurance are likely to be achieved. In the present study, due to the use of non-athletic postmenopausal women, it was not possible to increase the number of repetitions and the variety of movement patterns. Also, it has to be noted that participants in TRX exercises use their body weight as a strength, and this, especially in non-athletic postmenopausal women, caused the maximum number of repetitions recorded for movements at the specified intensity to be on average 8 repetitions.
ConclusionAdaptation to regular exercise reduces the symptoms of menopause. In this study, there was no significant difference between using different intensities of training. Therefore, due to the combined physiological and psychological aspects of menopause, it is probably the most important factor in improving menopausal symptoms in the first place is participating in exercise and the frequency of exercise. TRX can also be used as a method in different intensities in this group of women. Based on the findings of this study, menopausal women are recommended to use low, moderate, or high-intensity TRX exercises to minimize the negative effects of menopause, such as hot flashes, and to improve physical fitness factors such as muscular endurance. However, further studies are needed, especially in the field of sports biomechanics and sports pathology, as well as other variables related to sports physiology and training principles to examine the safety of these exercises for postmenopausal women as well as the elderly.
FundingNone.
Conflict of interestThe authors have no conflicts of interest to report.
The authors of this paper would like to express their thanks to all participants and Histogenotech research center (www.histogene.ir) especially for their critical comments during the project.

